


1Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, 2Department of Ophthalmology and Department of Pathology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark, 3Department of Clinical Neuroscience, Division of Ophthalmology and Vision, Karolinska Institutet, Stockholm, Sweden, 4Department of Skin and Allergic Diseases and 11Department of Dermatology, Helsinki University Central Hospital, Helsinki, Finland, 5Department of Dermatology, Bispebjerg University Hospital, Copenhagen, Denmark, 6Department of Dermatology/Allergology, University Medical Center Utrecht, Utrecht, The Netherlands, 7Hudpoliklinikken, Namsos, Norway, 8Department of Dermatology, Tampere University Hospital, Tampere, Finland, 9Dermatology and Venereology Unit, Department of Medicine, Karolinska University Hospital, Stockholm, Sweden, 10Department of Dermatology, Kainuu Central Hospital, Kajaani, Finland, 12Särnhult Tore, Hallandskustens Hudmottagning, Kungsbacka, Sweden, 13Department of Dermatology, Nordland Hospital, Bodø, 14Department of Pathology, Oslo University Hospital, Oslo, Norway, 15Department of Dermatology and Venereology, Åarhus University Hospital, Åarhus, Denmark, and 16Department of Dermatology, Skåne University Hospital & Clinical Research Centre, Lund University, Malmö, Sweden
There is a need for unified guidance on the management of ocular manifestations of atopic dermatitis and ocular manifestations associated with dupilumab in the Nordic region (Denmark, Finland, Norway and Sweden). This initiative gathered Nordic dermatologists and ophthalmologists to identify consensus in this area using a modified Delphi process. The initiative was led by a Nordic expert panel who developed a questionnaire that was circulated to a wider group. The results informed an agenda consisting of 24 statements to be voted on using a 5-point Likert scale at a meeting in Copenhagen on 24 April 2019. A facilitator moderated discussion and revised statements according to expert feedback for a second vote when required to reach consensus. Consensus was reached for 23 statements regarding the diagnosis, treatment and referral of these patients, which we hope will improve patient management in the Nordic region.
Key words: atopic dermatitis; consensus; modified Delphi process; ocular manifestation.
Accepted Sep 7, 2020; Epub ahead of print Sep 14, 2020
Acta Derm Venereol 2020; 100: adv00264.
doi: 10.2340/00015555-3629
Corr: Jacob P. Thyssen, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, Denmark. Email: jacob.pontoppidan.thyssen@regionh.dk
There is a need for guidance on the management of ocular manifestations of atopic dermatitis and ocular manifestations associated with dupilumab in the Nordic region (Denmark, Finland, Norway and Sweden). Nordic dermatologists and ophthalmologists worked together to identify consensus in this area, using a modified Delphi process, which involved voting on the extent to which the audience agreed with a series of statements. Consensus was reached for 22 of the 24 statements regarding the diagnosis, treatment and referral of these patients, which we hope will improve patient management in the Nordic region.
Atopic dermatitis (AD) is a chronic skin disease with pronounced type 2 inflammation that affects approximately 3–5% of adults and up to 20% of children worldwide (1–5). AD is associated with a broad spectrum of clinical presentations and severities, which may be influenced by a number of factors, such as age, environment and genetic predisposition (5); common co-morbidities include allergic rhinitis and asthma (6, 7). AD is also associated with ocular manifestations, of which there is currently limited awareness (8).
The anti-interleukin-4 receptor alpha monoclonal antibody dupilumab (9) has been approved in the USA (10) and Europe (11) for the treatment of AD in patients whose disease has not been adequately controlled with prior treatments or when other therapies are not advis-able. However, in patients with AD enrolled in 2 phase 3 studies, dupilumab was associated with increased risk of conjunctivitis compared with placebo (dupilumab 300 mg every other week (4%); dupilumab 300 mg every week (4%); placebo (1%)) (7). Frequent occurrence of conjunctivitis and blepharitis has also been reported in real-world use of dupilumab (12–15). It has been documented that the occurrence of dupilumab-associated ocular manifestations increases with severity of AD and is more common in individuals with a history of conjunctivitis (16–18). Symptoms commonly experienced by patients with AD receiving dupilumab include conjunctival redness, hyperaemia, blepharitis, dryness and discharge (19). The prominent features of dupilumab-associated conjunctivitis are the predominant involvement of the conjunctiva and hyperaemia of the limbus (18).
The pathogenesis of dupilumab-associated conjunc-tivitis is not yet fully understood, but is associated with a focal scarcity of intraepithelial goblet cells, which differs from the histopathology of allergic conjunctivitis (20, 21). Dupilumab-associated conjunctivitis is thought to be specific to patients with AD, as it is rarely experienced by patients receiving dupilumab for the treatment of asthma or nasal polyposis (20, 22). With the advent of new treatments, greater scrutiny of patients with AD and increased observation of the ocular events associated with dupilumab are warranted (7, 23).
Dermatologists have neither the facilities nor training in ophthalmic investigation to effectively diagnose ocular events and it is not a usual part of their patient workup; a view broadly consistent with that of the International Eczema Council (24). To ensure safe and optimum patient management, dermatologists need to understand how to recognize the signs and symptoms of the ocular manifesta-tions of AD and those that may be caused by treatment, how to treat, and when to refer patients to an ophthalmologist. As such, Sanofi Genzyme invited dermatologists and ophthalmologists from the Nordic region (Denmark, Finland, Norway and Sweden) to gather for a consensus meeting using a modified Delphi process to discuss the management of the ocular manifestations of AD, led by an expert group of dermatologists and ophthalmologists.
Expert panel and other meeting attendees
The expert panel, chosen and invited by Sanofi Genzyme, consisted of 3 dermatologists (Maria Bradley (Sweden), Anita Remitz (Finland) and Jacob P. Thyssen (Denmark)) and 2 ophthalmologists (Steffen Heegaard (Denmark) and Lena Ivert (Sweden)) with a particular interest in the management of patients with AD and relevant experience of the ocular events associated with dupilumab.
In addition to the expert panel, 12 dermatologists (3 each from Denmark, Finland, Norway and Sweden) and 1 ophthalmologist (from Norway) attended the meeting as advisors, all of whom had an interest in the management of patients with AD. Marjolein de Bruin-Weller, an expert dermatologist from The Netherlands, also participated in the meeting by providing a presentation on the management of ocular events associated with dupilumab (18). Individuals from Sanofi Genzyme were present during the meeting, but did not provide input on the discussions.
Modified Delphi process
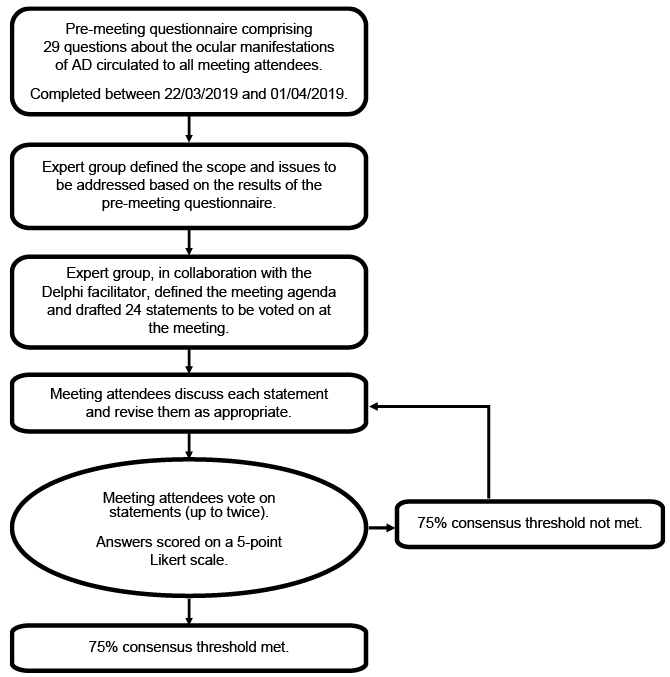
The Delphi process is a recognized facilitation technique used to gain consensus between specialists in a particular field where expert opinion is important in shaping judgements (Fig. 1) (25). This approach provides experts with an opportunity to alter their response based on their peers’ opinions, thus increasing the likelihood of the convergence of opinions. The expert group led the initiative by defining the scope of the issues to be addressed; this was informed by a pre-meeting questionnaire that was developed by the expert panel and distributed to all the meeting participants (this comprised 29 questions and was completed between 22 March 2019 and 1 April 2019). From this pre-meeting feedback, the expert group, in collaboration with the Delphi facilitator (Keena McKillen on behalf of OPEN Health Medical Communications), defined the meeting agenda and drafted 24 statements to be voted on at the meeting. The meeting took place on 24 April 2019.
Fig. 1. Modified Delphi process. AD: atopic dermatitis.
Voting to reach consensus
During the meeting, all Nordic experts voted on a series of statements about the management of the ocular manifestations of AD, moderated by an experienced Delphi facilitator and the possible answers scored on a 5-point Likert scale; in each instance, the experts could select only one answer. During the meeting, responses were captured using audience-response voting systems (provided by Crystal Interactive, Godalming, UK); this methodology provided anonymous answers and allowed the voting to be stratified by country of origin and specialty. All responses were reviewed and discussed regardless of the level of consensus obtained. If a consensus was not reached, experts participated in a detailed facilitated discussion to identify reasons for the lack of agreement. When warranted, the Delphi facilitator revised the statements according to the expert feedback and re-voting then occurred (for a maximum of 2 votes). A consensus threshold of 75% was pre-specified, consistent with recent consensus initiatives (26).
Atopic dermatitis and the eye: a guide for dermatologists
It was agreed that dermatologists should be aware of several ocular manifestations, including allergic conjunc-tivitis, blepharitis, eyelid eczema, keratoconjunctivitis, ocular surface infections, glaucoma and cataract secondary to corticosteroid treatment and keratoconus, although it was noted by the ophthalmologists that keratoconus is rare in patients with AD in the Nordic region (Table I). The ophthalmologists also advised caution when diagnos-ing conditions that have other possible diagnoses, such as rosacea for red eyes and allergic contact dermatitis for eyelid and periorbital eczema. Both the dermatologists and ophthalmologists agreed on the importance of dermatologists asking their patients with AD whether they have any eye complaints, because patients may not freely volunteer information about their eyes in response to general health questions, as they may think dermatologists are only concerned with skin complaints. When asking patients about conditions such as rhinoconjunctivitis, the importance of using patient-friendly terms, such as “hay fever”, was mentioned.
Table I. Atopic dermatitis (AD) and the eye: a guide for dermatologists
It was noted that dermatologists should be aware of the ocular signs and symptoms of AD and know when to refer patients to an ophthalmologist. The “red flag” ocular signs and symptoms for which dermatologists should be vigilant are presented in Table II. In symptomatic patients, it was agreed that dermatologists should conduct clinical examinations for conjunctival redness (Fig. 2a, b), eyelid eczema and signs of blepharitis.
The meeting attendees agreed that it would be appropriate for dermatologists to treat mild allergic conjunc-tivitis, blepharitis and eyelid eczema, but the participating ophthalmologists recommended that patients with more severe allergic conjunctivitis are referred to an ophthalmologist (Fig. 2). The ophthalmologists also noted that dermatologists should describe the following ocular signs and symptoms to patients so they can identify them and seek medical help as needed: blepharitis, conjunctivitis, discomfort, dry eyes, eye itching, pain, photophobia, redness, reduced visual acuity and tearing.
Table II. Red flags (warning signs)
Fig. 2. Three typical patients with ocular manifestations of atopic dermatitis that should be referred to an ophthalmologist. Patient one: (a) moderate conjunctivitis in the right eye, and (b) a more severe conjunctivitis in the left eye. Patient two: (c) a keratoconus due to atopic dermatitis, a herpes simplex keratitis as well as Staphylococcus aureus keratitis prior to uveitis with secondary glaucoma. The greyness paracentrally on the cornea was the stromal opacification due to the deep keratitis as well as temporary vessel ingrowth and conjunctival injection. Patient three: (d) severe conjunctivitis with signs of symblepharon development.
Management of ocular manifestations of atopic dermatitis in the dermatology clinic
The participating ophthalmologists reassured the dermatologists that the risk of increased intraocular pressure in patients using corticosteroid eye ointment on the eyelid is low (27), except in those patients who are corticosteroid sensitive. Moreover, dermatologists expressed concern about the long-term use of corticosteroid eye drops that necessitate close follow-up, which is often difficult in busy university hospitals. The ophthalmologists recommended a very conservative approach, which was to consider treating conjunctivitis with low-potency topical corticosteroids, such as hydrocortisone sodium phosphate (3.35 mg/ml eye drops, up to 3 times daily for 2 weeks) (except in patients with glaucoma, a history of previous corticosteroid-induced intraocular pressure elevation or a history of clinically relevant viral infections) and frequent use of preservative-free lubricating eye drops. The ophthalmologists then recommended that if patients still required treatment for conjunctivitis after 2 weeks of corticosteroid treatment that they should be referred to an ophthalmologist (Table III).
Table III. Management of ocular events in the dermatology clinic
It was recommended that dermatologists refer patients with moderate-to-severe blepharitis to an ophthalmologist. Whilst the patient is waiting for their consultation with an ophthalmologist, dermatologists should prescribe corticosteroid eye ointment (the combination of oxytetracycline and hydrocortisone is preferred, with the addition of polymyxin B) to be administered up to 3 times daily for 2 weeks (except in patients with glaucoma, a history of corticosteroid-induced intraocular pressure elevation or a history of clinically relevant viral infections). In patients with a history of corticosteroid-induced intraocular pressure elevation or glaucoma, topical calcineurin inhibitors, such as cyclosporine, 1 mg/ml, eye drops, are an appropriate treatment for long-term dupilumab-induced atopic conjunctivitis. However, as topical calcineurin inhibitor treatment is often associated with a burning sensation that causes low treatment compliance, it was recommended that these patients can also receive oxytetracycline and polymyxin B without concomitant hydrocortisone.
The ophthalmologists also noted that the barrier func-tion of the eye surface may be affected by AD; therefore, in addition to prescribing topical calcineurin inhibitors for the treatment of periorbital eczema or eyelid eczema, it is appropriate to consider prescribing concomitant preservative-free lubricating eye drops to alleviate discomfort from dry eyes. In some patients, topical calcineurin inhibitors have been documented to be associated with pain when administered on the eyelid, but not with increased intraocular pressure (28). Topical calcineurin inhibitors are used frequently as an alternative to topical corticosteroids to treat periorbital or eyelid eczema.
Management of ocular events associated with dupilumab
Owing to the increased risk of ocular events associated with dupilumab, it was noted that dermatologists should inform patients about the risk and/or provide patient information sheets that increase patient awareness of ocular signs and symptoms to empower them to seek treatment early. Both the dermatologists and ophthalmologists agreed that dermatologists should encourage patients to use lubricating eye drops 3–5 times per day, based on clinical judgement, even though there is no evidence in the literature at this time to support their efficacy in patients treated with dupilumab. This is worthy of further evaluation. Both the dermatologists and ophthalmologists also agreed that dupilumab-associated ocular manifestations, such as prolonged/severe conjunc-tivitis, blepharitis and redness, are the main diagnoses/signs and symptoms that should lead to referral to an ophthalmologist. Dermatologists should be vigilant for hyperaemia of the limbus (i.e. increased redness around the cornea), which is common in patients with conjunc-tivitis who are receiving dupilumab and is non-specific to allergic conjunctivitis.
Owing to increasing understanding of the ocular mani-festations of AD, the participating dermatologists and ophthalmologists also determined that it will be essential to develop pragmatic, flexible cross-disciplinary patient management plans that can be adapted to across different healthcare systems.
Education of other healthcare professionals and patients
There was no consensus on whether patients with AD should be given specific information about which healthcare professional should be contacted first if they experience an ocular manifestation. The dermatologists noted that patients may contact their GP about eye complaints as they are likely to be the healthcare professional with whom they have built the strongest relationship; their GP would then refer the patient to a specialist as appropriate. However, as many GPs are not familiar with dupilumab-associated conjunctivitis it could be misdiagnosed as rhinoconjunctivitis, which could delay appropriate treatment. The meeting attendees agreed that patients receiving dupilumab could contact their dermatologist if they experienced an ocular manifestation, as their dermatologist was the prescribing clinician; alternatively, if the patient is already consulting with an ophthalmologist, the ophthalmologist should be the first point of contact (Table IV).
Table IV. Key information to communicate to other healthcare professionals and patients
As the group agreed that patients receiving dupilumab should be told to inform their ophthalmologist of the possibility of ocular manifestations, it was suggested by the dermatologists and ophthalmologists that a leaflet detailing the possible ocular manifestations associated with dupilumab would be useful and should be developed and given to patients. A data-capture form was presented at the meeting that was used for the standardized examination of patients with dupilumab-associated ocular events during dupilumab clinical trials in Utrecht, The Netherlands and Munich, Germany (Fig. S1). The form increases awareness of dupilumab-associated ocular events, such as limbal oedema and limbitis; dermatologists provide the form to patients upon referral to an ophthalmologist.
Lastly, in the context of the lower occurrence of ocular events in patients without AD who were treated with dupilumab (7), the meeting attendees agreed that allergists, GPs, paediatricians, pharmacists and pulmonologists should also be educated about the ocular manifestations associated with AD and dupilumab treatment.
A modified Delphi process was used to achieve consensus owing to the absence of comprehensive and country-specific guidance on the management of the ocular manifestations of AD. As the underlying mechanisms of the ocular manifestations of AD and the ocular events associated with dupilumab are only beginning to be understood, clinical judgement and insight are required to guide the clinical practice of dermatologists given the growing pool of scientific data.
This consensus approach was limited by the relatively low number of attending experts and advisors. The experts and advisors were from 4 countries in the Nordic region, therefore, our recommendations may not be applic-able in other parts of the world. Clinicians in the region have limited experience with managing patients who are receiving dupilumab because it has only recently been approved by the European Medicines Agency (EMA) for the treatment of AD. In addition, although the modified Delphi process is an accepted methodology, it is based on expert opinion and open to possible bias in responses. Finally, the pathogenesis of dupilumab-associated conjunctivitis is not yet fully understood (24, 29, 30) and we did not include discussions on potential exposures that could influence decisions, e.g. contact lenses and use of other eye drops.
In conclusion, currently, there is an unmet need for unified clinical guidance on the management of the ocular manifestations of AD. Our consensus meeting provides broad recommendations on the diagnosis, treatment and referral of patients with ocular manifestations of AD and it should be used as a framework to facilitate further collaboration between dermatologists and ophthalmologists; these recommendations provide wider education to better support patient management in this developing area.
Written informed consent for publication of the clinical images in Fig. 2 was obtained from the patients.
Medical writing support was provided by Matthew Reynolds from OPEN Health Medical Communications, funded by Sanofi Genzyme. Keena McKillen, on behalf of OPEN Health Medical Communications, was the Delphi facilitator.
This study was funded by Sanofi Genzyme.
Conflicts of interest: JPT has been an advisor/speaker/investigator for Abbvie, Pfizer, Regeneron, Sanofi-Genzyme, Eli Lilly and LEO Pharma. SH reports personal fees from Sanofi during the conduct of the study. LI reports no conflicts of interest. AR received compensation for clinical studies from Regeneron/Sanofi, Lily and Novartis, and personal fees for lectures from Leo Pharma. TA reports grants, personal fees and non-financial support from Sanofi. Md B-W reports grants and personal fees from Regeneron/Sanofi-Genzyme during the conduct of the study; personal fees from AbbVie for consultancy and PI multicentre studies, personal fees from Pfizer for consultancy and PI multicentre studies, personal fees from Leo Pharma for consultancy and PI multicentre studies, personal fees from UCB for consultancy and from Galderma for consultancy outside the submitted work. All fees are paid to the University Medical Center Utrecht, the Netherlands. TH-N reports personal fees and non-financial support from Sanofi Norway for lecturing during the conduct of the study and personal fees from Sanofi Norway for travel and stay outside the submitted work. LK reports non-financial support from Sanofi Genzyme during the conduct of the study and non-financial support from Abbvie, personal fees and non-financial support from Novartis, personal fees from Orion, personal fees, non-financial support and other from Sanofi Genzyme outside the submitted work. LUI reports financial support from Sanofi Genzyme for lecturing outside the submitted work. PL reports personal fees from Sanofi Genzyme for consultancy and non-financial support from Sanofi Genzyme for travel during the conduct of the study. JM reports non-financial support from Sanofi Genzyme during the conduct of the study and personal fees from Sanofi Genzyme for consultation, personal fees from Orion Pharma for lecturing, non-financial support from Medac for travel outside the submitted work. TS reports no conflicts of interest. TS has received refund for travel expenses as well as personal fees for consulting from Sanofi. ES reports personal fees from Sanofi Genzyme for consultancy during the conduct of the study. SFT reports personal fees from Sanofi for an advisory board during the conduct of the study and grants from Sanofi for research support outside the submitted work. TT reports personal fees from Sanofi Genyzme for an advisory board during the conduct of the study. CV reports travel grants from Sanofi during the conduct of the study, as well as grants and personal fees from Sanofi outside the submitted work. LvK reports grants and participation in advisory boards. MB has received grants funding from Sanofi-Genzyme, speaker honoraria from Novartis, AstraZeneca, AbbVie, Leo Pharma and Celgene and has attended advisory boards for Sanofi-Genzyme, Novartis, Lilly, AbbVie and Leo Pharma.


 Click to show fullsize
Click to show fullsize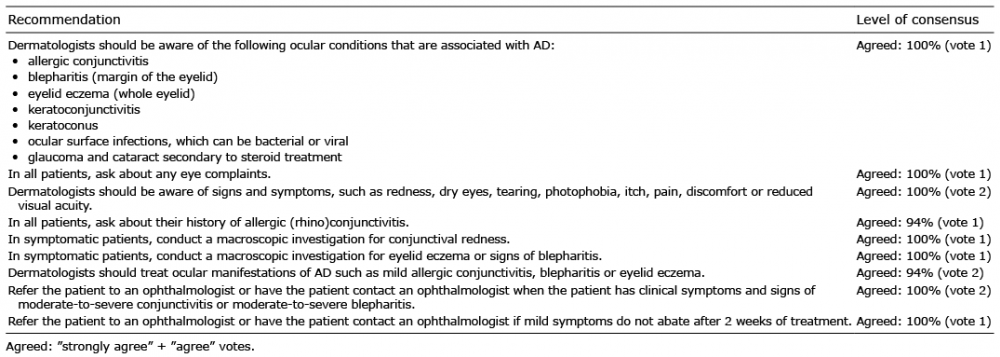 Click to show fullsize
Click to show fullsize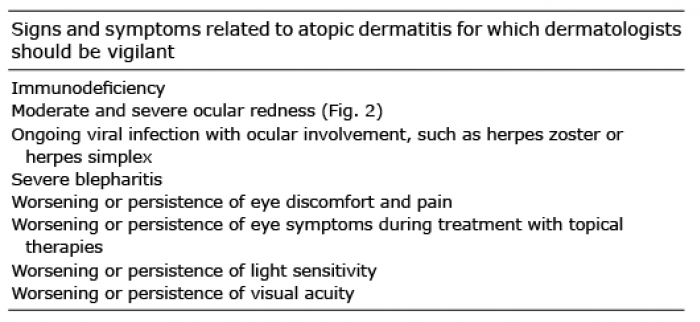 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize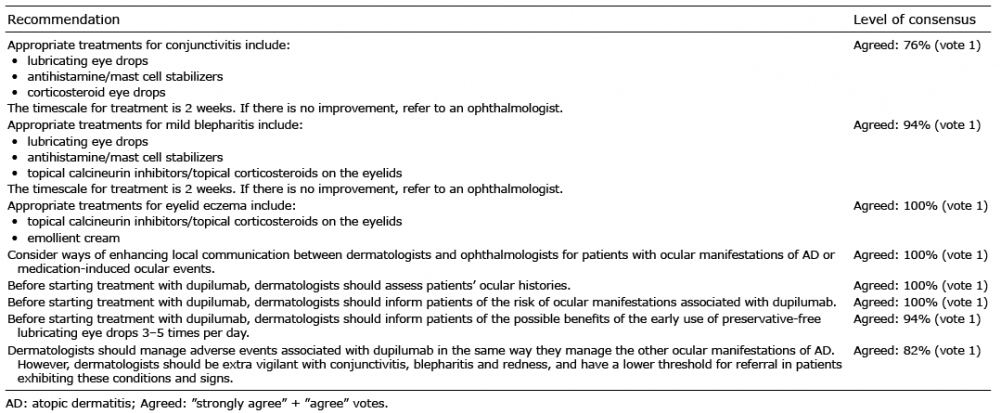 Click to show fullsize
Click to show fullsize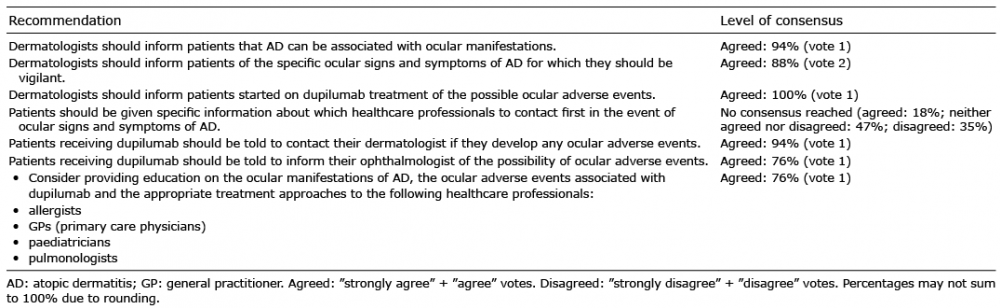 Click to show fullsize
Click to show fullsize